In this section : Haematology and Thrombosis
Myeloma
Warfarin
Anticoagulation for AF, DVT and PE
Orthopaedic VTE Risk Assessment
Haemolytic Anaemia
Platelet Transfusion
Parenteral Iron in Adults >18 Years
Pulmonary Embolism
Deep Vein Thrombosis of Lower Extremities
Bleeding with Other Antithrombotics
Low Molecular Weight Heparin
Haematinic Testing
Thromboprophylaxis for Non-Covid Patients
Thrombophilia Screening
Antithrombotics in Hip Fracture
Reversal of Warfarin
Lumbar Puncture, Antiplatelet & Anticoagulant Drugs
Antithrombotics & Surgery
Iron Deficiency Anaemia
Unfractionated Heparin Infusion
Massive Pulmonary Embolism
Unfractionated Heparin Infusion
Last updated 3rd December 2020
Recommended in Following Situations
- Used in treatment of DVT / PE if rapid anticoagulation is deemed appropriate (e.g. massive PE) or patients thought to be at particularly high bleeding risk (e.g. recent surgery/trauma).
Before Starting Unfractionated Heparin
- Check for contraindications to heparin as below:
- Allergy to Heparin
- History of Heparin induced thrombocytopenia
- Coagulopathy
- Therapeutic anticoagulation
- Known bleeding disorder
- Active bleeding/Suspected bleeding
- New haemorrhagic CVA, ? New thrombotic CVA (discuss with Consultant)
- Pericarditis
- Severe hypertension SBP >180 or DBP >110
- Low platelet count <60
- Patient on ICP for dying (discuss with Consultant)
- Ensure baseline platelet count, clotting screen, renal function tested and results checked.
Loading Dose
- If no contraindications, prescribe on “once only” section of medicine chart as “Heparin Loading Dose as Charted”
- Rx 5,000 units by IV bolus over 5 minutes – use one 5 ml vial of 1000 units/ml (total concentration 5000 units/5 ml)
- If patient at high risk of bleed, discuss risks/benefits with Consultant. If decision made to treat then consider omitting loading dose and start at 1000units/hour irrespective of weight. Patient with massive PE may still need standard dosing.

Maintenance Infusion
- Rx 18 units/kg/hour (rounded to the nearest 100 unit dose and NOT EXCEEDING 1800 UNITS/HOUR), prescribed on Medicine Chart as “Heparin Sodium 20,000 units in 20ml as charted”.
- Draw up contents of one ampoule of 20,000units in 20ml Heparin sodium in a syringe for infusion via a syringe pump. This preparation does not require further dilution.

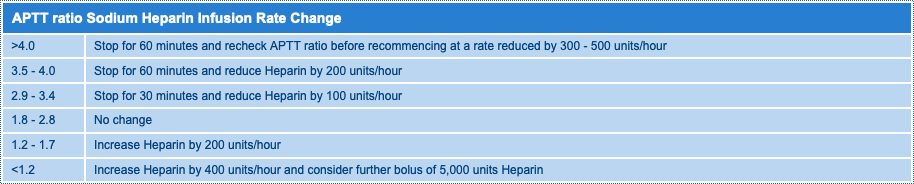
Check APTT Ratio 4 hours After Starting Treatment
- Adjust infusion rate to nearest 100 unit dose according to table.
Monitor Platelet Count
- Platelet count monitoring for heparin induced thrombocytopenia (HIT) should be performed if there has been exposure to heparin (LMWH or UFH) in past 3 months or if UFH is to continue beyond 5 days.
What to do if Patient Bleeds on IV Heparin
- Stopping Heparin is almost always sufficient.
- The anticoagulant effect of unfractionated Heparin is reliably and rapidly reversed using protamine sulphate.
- To antagonise a heparin infusion, stop the heparin then Rx 25-50mg protamine as a slow IV injection at rate not >5mg/min to minimise side effects eg hypotension, bradycardia & flushing
- Not more than 50mg protamine should be given in a 10 min period. Higher doses can have an anticoagulant effect.
- Protamine sulphate can cause hypersensitivity reactions and should be used with caution in patients treated previously with protamine or protamine insulin preparations (Isophane insulin) or fish allergy.
- Ensure resus facilities available when protamine given
- Check APTT 30min after protamine. Consider further doses if patient still bleeding and APTT still prolonged.