In this section : Respiratory
Croup
Bronchiolitis
Acute Wheeze or Asthma in Paediatrics
Inhalers for Adults with Asthma
Greener Inhaler Prescribing
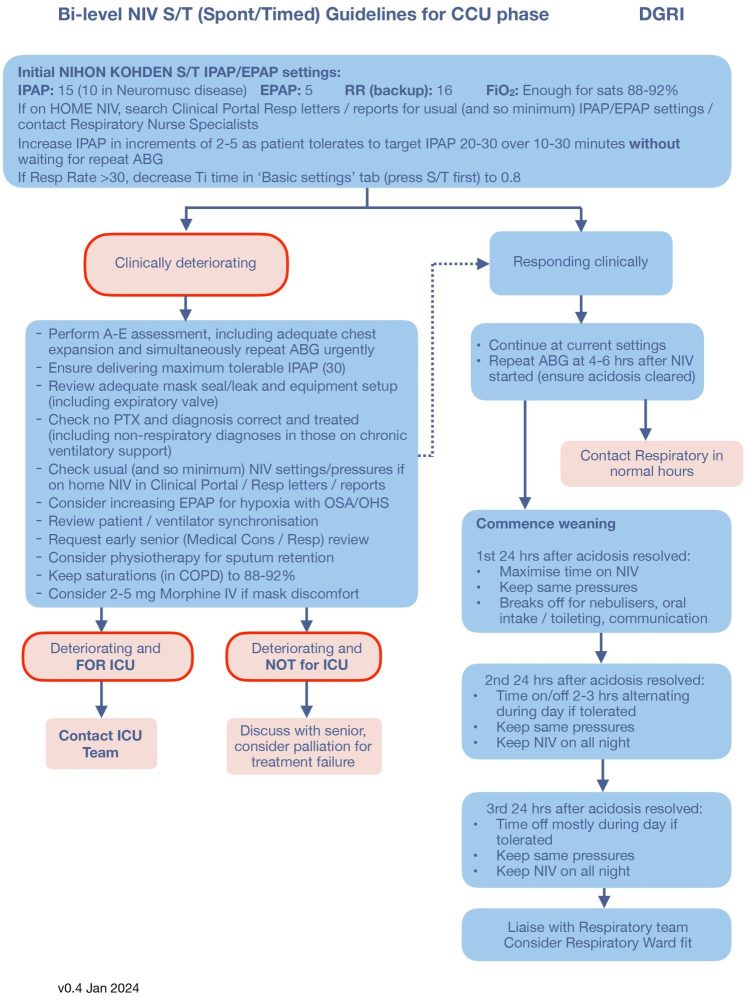
Bi-Level NIV S/T Guidelines for CCU Phase
Bi-Level NIV S/T Guidelines for ED Phase
Chronic Cough Pathway
Paediatric Bronchiolitis
Exacerbation of COPD
Chronic Obstructive Pulmonary Disease
Legionnaires Disease
Interstitial Lung Disease
Oxygen Therapy
Acute Asthma
Pleural Effusion
Spontaneous Pneumothorax
Community Acquired Pneumonia (CAP)
Breathlessness with Abnormal CXR
Home | Articles | Respiratory |
Bi-Level NIV S/T Guidelines for CCU Phase
Last updated 4th March 2024
Content updated by Dr Alex McDonald