In this section : Vascular
Abdominal Aortic Aneurysms
Abdominal Aortic Aneurysms
Last updated 15th March 2024
Epidemiology and Risk Factors
- AAA most often occur in the aorta between the renal and inferior mesenteric artery
- A diameter >3.0cm is considered aneurysmal
- Very uncommon before age 55 years, then increases dramatically with age.
- 4-5 times more common in men
- Other risk factors include smoking, hypertension, family history and vascular disease at other sites
Clinical Presentation
- Most aneurysms remain quiescent until rupture
- An enlarging aneurysm may cause abdominal or back pain and may be tender to palpation
- Most are detected as an incidental finding on sonar, CT or MR
- Approx 30% are discovered when a pulsatile abdominal mass is palpated on routine examination
Imaging
- Sonar is preferred modality for screening and for assessing and following AAA – see below for screening intervals.
- CT is preferred for surgical planning and suspected rupture, but is too expensive for screening. CT measurements are on average 0.3-0.9cm larger than ultrasound measurements
Ruptured AAA
- Classically presents with abdominal or back pain, hypotension and a expansile abdominal mass
- If BP relatively stable then aneurysm rupture has been temporarily contained by the surrounding retroperitoneum
- AAA rupture may mimic ureteric colic, pancreatitis, acute coronary syndrome, a biliary tract disease – do not diagnose a first attack of ureteric colic in patient >55 years.
Investigation and Management
- If patient has survived long enough to reach A&E then refer immediately to surgeons
- In many cases the diagnosis is clinical and patient may go directly to theatre
- If imaging required this should be CT not ultrasound
- Insert 2 large bore cannulae and give high flow oxygen
- Restore SBP to 100mmHg not more with IV fluids
- Take blood for FBC, U&E, LFT and cross match 6 units
- The local vascular surgeon will operate or the local on call general surgeon will refer to the solway vascular service
Small Aneurysms 3.0-5.5cm
- These are usually picked up as an incidental finding when patient is having abdominal sonar for other reasons
- Refer to Vascular Lab in Ward 5 on first floor for surveillance, by letter or by phone call to Shirley Wight, Vascular Nurse Specialist, on 33833
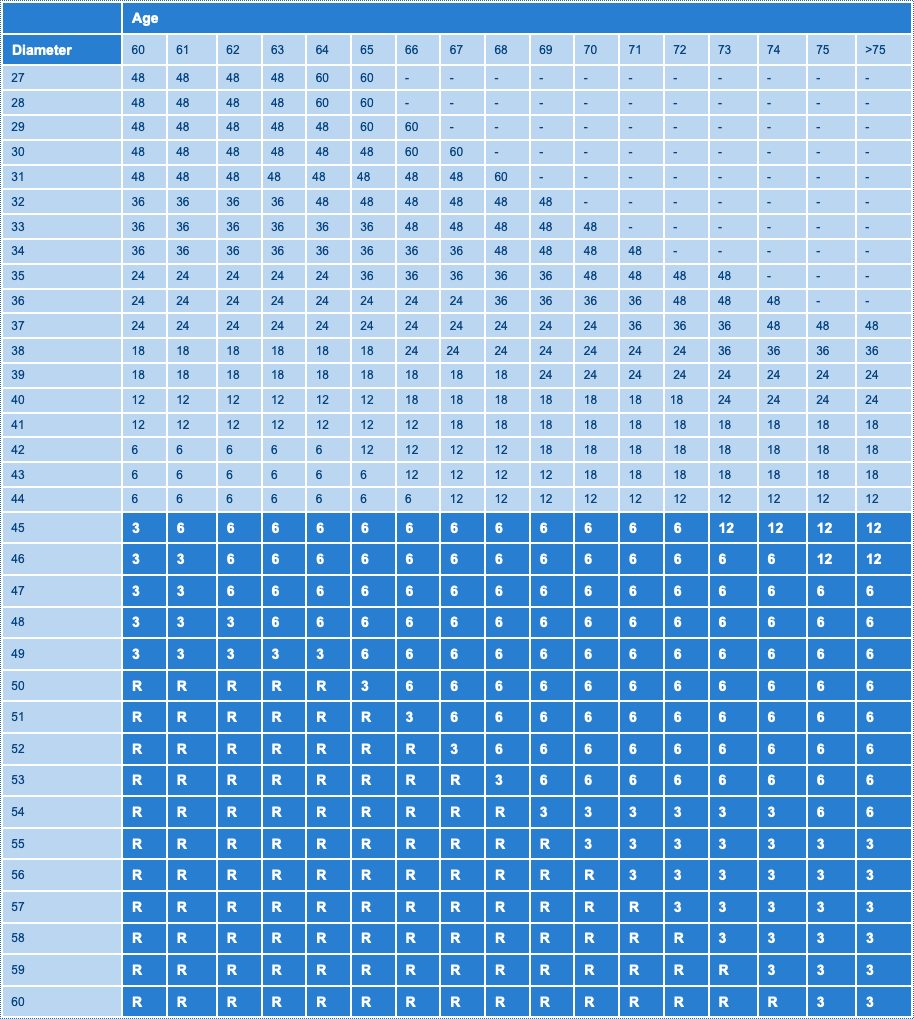
Interval Between Scans for Monitoring Aortic Growth
- The table suggests when to scan, (rescan interval in months), when to refer to vascular surgeon (shaded) and when to consider for elective repair (R).