In this section : Death Certification
Death Certification
Confirmation of Death
Death & The Procurator Fiscal
Autopsies
Home | Articles | Death Certification |
Death Certification
Last updated 27th February 2024
Introduction
- A Medical Certificate of Cause of Death (MCCD) is a statutory requirement. It enables the family to register the death, make arrangements for a funeral and settle the estate of the deceased.
- It isn’t always completed correctly, leading to delays for families at a time when they would like everything to run smoothly.
- The MCCD should be done within one working day unless Procurator Fiscal referral is required (https://www.copfs.gov.uk/for-professionals/reporting-deaths/). Speak to a senior doctor or the patient’s consultant if this may be required.
- If you think having been in contact with the family, that they may benefit from the further examination of the body by hospital post-mortem (if not a Fiscal case), seek senior doctor advice at the time of speaking to the family (8am-9pm) or the next day.
- You don’t have to have looked after the patient to complete the MCCD if the cause of death is obvious from the notes.
- If death occurs out of hours on downstream medical wards, the MCCD should wait for the next working day and be completed by the day team, if necessary after discussing with the patient’s consultant if the cause of death is unclear.
- If death occurs In AMU between 0800 and 2100, on any day of the week, you should speak to the patient’s consultant or the duty consultant if the cause of death is unclear.
- If the doctor who certifies the death does not complete the MCCD, then he or she is responsible for handing it over to the parent team.
- There is an excellent resource on death certification which you can access via this link. Support Around Death – Death Certification
- We suggest you familiarise yourself with the documents listed in the panel on the left hand side of the home page, especially Parts A to E.
- To access the module Death Certification: Identifying Common Mistakes, you will need to log in to your TURAS:Learn account.
Completion of the Medical Certificate of Cause of Death (MCCD)
- Do not keep the ward waiting.
- Check you have the right patient.
- View the body to confirm death. If the body is already in the mortuary check that the death has been confirmed and documented legibly in the notes.
- Write the causes of death as per the certificate in the patient’s notes and also write the certificate number alongside this.
- We recommend the Learnpro Module ‘NES: Death Certification: Identifying Common Mistakes’.
- Note that separate cremation forms are no longer required.
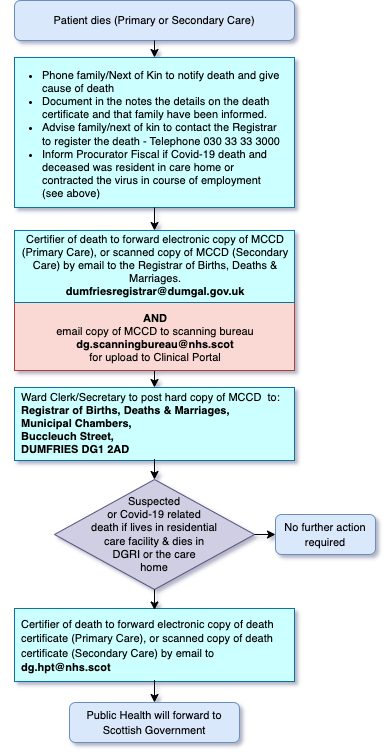
- Since the beginning of the COVID-19 pandemic we no longer hand MCCDs to relatives but you should phone them instead to let them know the certificate has been completed. Our ward administration team will email the Registrars direct and post the paper copy to the Registrar.
- Remember to introduce yourself when phoning relatives, offer sympathy, explain the content of the MCCD and say that a small number of certificates may be selected for review by the MCCD Review Panel. If the MCCD is selected for review but the family would like the funeral to go ahead you can apply for advance registration which means that the funeral can take place before the review has been completed.
- If you are not available to receive a call from the medical reviewer should the certificate be selected for review, your colleagues MUST be able to state and justify your entry.
- For further advice on what to do next and also if patient has died with confirmed or suspected COVID-19 Click here.
What You Can and Cannot Write on Death Certificate
- Print clearly avoiding abbreviations to reduce difficulties Registrars have in deciphering illegible handwriting.
- Be specific eg for colon cancer, specify rectal, sigmoid, ascending, descending or transverse colon. If primary not known say so eg ‘carcinomatosis – primary not known’.
- Avoid giving mode of death only eg asphyxia, asthenia, cachexia, coma, exhaustion, shock, syncope, unless further qualified eg ‘coma due to cerebral haemorrhage’.
- Avoid ill defined terms eg cardiac, renal, hepatic or respiratory failure unless further qualified eg ‘cardiac failure, secondary to ischaemic heart disease’ or even ‘cardiac failure- cause unknown’.
- Complete the counterfoil for reference purposes
- The current guidance on what you can and cannot write is available by clicking this link www.sehd.scot.nhs.uk/cmo/CMO(2009)10.pdf
What to do Next
- Once you have completed the MCCD this should be scanned and emailed to the registrar (registration of birth, death and Marriages office via: [email protected]).
- You should also email a copy of the MCCD to the Scanning Bureau ([email protected]) for uploading to Clinical Portal.
- The hard copy of the MCCD must be posted to the registrar. Please ensure this is handed to the ward co-ordinator or nurse in charge if out of hours.
- If a MCCD has to be re-issued and emailed to the registrar, the new MCCD should be printed and given to the ward clerk for uploading to the clinical portal.
- If a MCCD has to be amended following discussion with the registrar, the e-mail correspondence should be printed and given to the ward clerk for uploading to the clinical portal.