In this section : Haematology and Thrombosis
Myeloma
Warfarin
Anticoagulation for AF, DVT and PE
Orthopaedic VTE Risk Assessment
Haemolytic Anaemia
Platelet Transfusion
Parenteral Iron in Adults >18 Years
Pulmonary Embolism
Deep Vein Thrombosis of Lower Extremities
Bleeding with Other Antithrombotics
Low Molecular Weight Heparin
Haematinic Testing
Thromboprophylaxis for Non-Covid Patients
Thrombophilia Screening
Antithrombotics in Hip Fracture
Reversal of Warfarin
Lumbar Puncture, Antiplatelet & Anticoagulant Drugs
Antithrombotics & Surgery
Iron Deficiency Anaemia
Unfractionated Heparin Infusion
Massive Pulmonary Embolism
Antithrombotics in Hip Fracture
Last updated 15th January 2024
Consensus Statement for Management of Anticoagulants and Antiplatelet Drugs in Patients with Hip Fracture
- Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
- Delaying surgery leads to complications such as pneumonia, pressure sores and increased mortality.
- This consensus statement has been written with the intent of giving practical advice on the management of anticoagulants in hip fracture patients so that surgery can proceed safely with the minimum possible delay.
- It is intended as a guideline only, and may be a useful framework should individual Health Boards wish to develop their own, local guideline.
Key issues for the Emergency Department (ED)/Ward
- Make a plan for management of anticoagulation on admission – do not delay this until the ward round the next day.
- Withhold anticoagulant and document timing of last dose of anticoagulant.
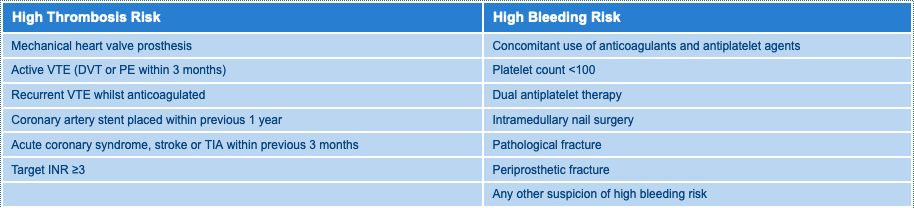
- If HIGH THROMBOSIS RISK* (second table below) then bridging anticoagulation may be required. Discuss with on-call haematologist, and inform on-call anaesthetist.
- Follow Drug Specific Advice below.
- Reverse warfarin on admission. Delay in reversal may delay surgery. Use of vitamin K and beriplex is detailed below.
- Do not give pre-operative prophylactic-dose dalteparin to anticoagulated patients.
- Delaying surgery because of anticoagulation should only be considered when the risk from bleeding outweighs the poorer survival associated with delay
- NSAIDs will increase the bleeding risk in patients taking anticoagulants and are not advised in this patient group.
- Fascia iliaca blocks are relatively low risk of bleeding and, as such, may be considered in anticoagulated patients. Considerations should be made to bleeding risks and benefit from better analgesia, and a risk/ benefit decision made with the patient on a case by case basis.
Intra-Operative Care
- Remember some residual anticoagulant effect may persist, and bleeding risk may be increased.
- Avoid neuraxial anaesthesia unless you are certain anticoagulation has been reversed (i.e. INR <1.5 if on warfarin). Neuraxial anaesthesia may be used in patients on aspirin monotherapy but is relatively contraindicated in patients on dual antiplatelet therapy and clopidogrel monotherapy.
- Note that, in patients taking Direct Oral Anticoagulants (DOACs), an INR measurement of <1.5 does not indicate a safe level of anticoagulation to allow surgery or regional anaesthesia.
- Tranexamic acid reduces bleeding with anticoagulants and 1g IV should be considered for all patients, and be given upon induction by the anaesthetist. Do not use in patients with Disseminated Intravascular Coagulation.
Post-Operative Care
- Prophylaxis-dose LMWH or Fondaparinux should be commenced not less than 6 hours after surgery, and continued until therapeutic anticoagulation achieved (e.g. INR within therapeutic range, DOAC recommenced).
- Restart anticoagulant 24-48 hours post-operatively if wound is dry. warfarin can be restarted at usual maintenance dose. If clopidogrel has been withheld it should be restarted 24 hours post-op (assuming haemostasis).
Reversing Warfarin
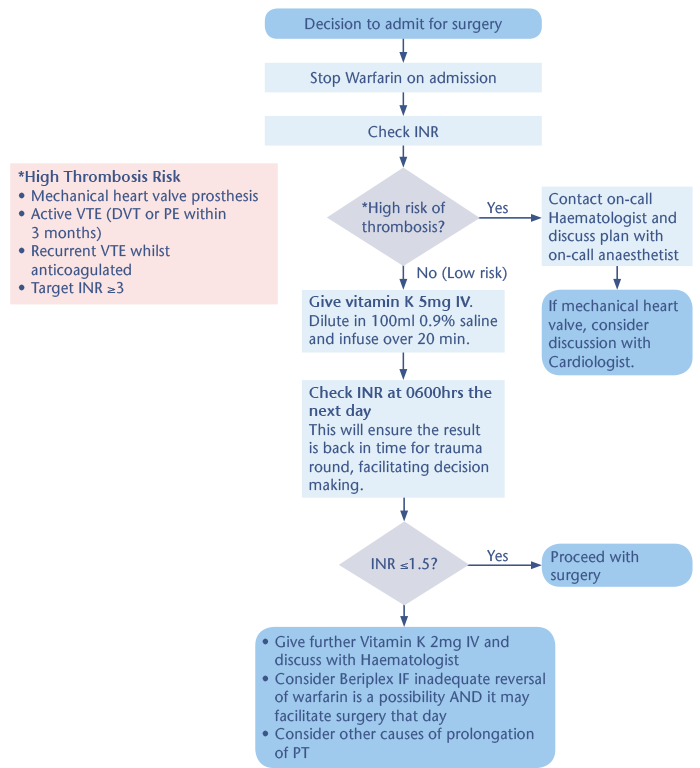
- Check INR on admission.
- If the patient is not at high thrombosis risk* then give 5mg vitamin K intravenously as soon as possible (e.g. in ED). Give as infusion diluted in 100ml 0.9% saline over 20 minutes.
- Plan surgery for the day after admission.
- Check INR at 6am on day of surgery so that result is back for the ward round.
- Proceed with surgery if INR ≤1.5.
- If INR still >1.5 then do not remove from operating list; aim to rapidly correct coagulation so surgery can proceed by giving a further vitamin K 2mg IV and recheck INR 4 hours later.
- Beriplex will rapidly reverse warfarin and is indicated if surgery on that day would otherwise be cancelled due to incomplete reversal of warfarin. Discuss with orthopaedic/anaesthetic consultant.
- Warfarin anticoagulation must be actively reversed. ‘Spontaneous reversal’ without active treatment is slow, unpredictable, does not reduce thrombosis risk, and unacceptably delays surgery.
- Do not use fresh frozen plasma for reversal of warfarin as reversal is slow, has a high volume, and exposes the patient unnecessarily to blood components.
Restarting Warfarin in Low Risk Patients
- Start dalteparin prophylaxis dose as per local VTE guidelines.
- If there are no wound complications then restart warfarin at usual dose 24 hours post-operatively.
- Check INR daily; continue dalteparin until INR within target range.
Heparins
- LMWH Prophylaxis dose e.g. dalteparin 5000 unit S/C, enoxaparin 40mg S/C – Plan surgery 12 hours from last dose.
- LMWH Treatment dose e.g. dalteparin >prophylaxis dose, enoxaparin 1mg/ kg BD – Plan surgery 24 hours from last dose. Surgery may be considered at 12-24 hours post-dose, however risk of bleeding is increased and neuraxial anaesthesia is contraindicated.
- Unfractionated heparin VTE prophylaxis e.g. heparin 5000 unit S/C BD – Plan surgery 4 hours from last dose.
- Unfractionated heparin by infusion. – Plan surgery 4 hours after cessation of infusion and check aPTT may be considered if at high risk of bleeding but is not usually required.
Direct Oral Anticoagulants (DOACs)
- Stop DOAC medicine on admission.
- Ascertain timing of last dose of DOAC and estimate bleeding risk. Use the table below to plan timing for surgery. Estimate time of surgery from last dose of anticoagulant, not time of admission to hospital.
- Estimate renal function. DOACs accumulate in renal failure so GFR should be measured, using either eGFR estimation or creatinine clearance calculation (such as Cockcroft Gault). The latter is preferred although eGFR may give an adequate estimation of renal function in patients out with extremes of body size.
- Standard clotting tests (PT, aPTT, INR) cannot be used for measuring anticoagulant effect from dabigatran, rivaroxaban, apixaban and edoxaban. Specifically calibrated anti-Xa assays can be used for rivaroxaban, edoxaban and apixaban, and should only be used at the request of a haematologist. Dabigatran can only be measured with dilute thrombin time (dTT) and not other clotting tests.
- Dabigatran can be reversed with idarucizumab (Praxbind) and may be indicated if delay to surgery is predicted to be >24-48 hours (see table 1 below). Discuss with haematologist. A specific reversal agent for –aban drugs is in development but not yet available.
- Neuraxial anaesthesia is best avoided unless residual DOAC effect can be excluded e.g. by calibrated anti-Xa assay.
- If no wound complications then restart DOAC 24-48 hours post-operatively.
Time from Last Dose of Anticoagulant to Surgery
| Standard Bleeding Risk | |||
|---|---|---|---|
| CrCl greater than 30 | CrCl less than 30 | High Bleeding Risk | |
| Apixaban | 24 hours from last dose | 48 hours from last dose | Extended time by 24 hours |
| Rivaroxaban | 24 hours from last dose | 48 hours from last dose | Extended time by 24 hours |
| Edoxaban | 24 hours from last dose | 48 hours from last dose | Extended time by 24 hours |
| Dabigatran | CrCl>80: 24h delay CrCl 50-80: 24-48h delay CrCl 30-50: 48-72h delay | Extended time by 24 hours | |
Aspirin
- Continue aspirin and proceed to surgery without delay
Clopidogrel
- If not high risk of bleeding then continue clopidogrel and proceed to surgery without delay.
- If high risk of bleeding withhold for 24 hours pre-operatively and then proceed to surgery.
- Evidence suggests a non-significant trend towards increased bleeding risk but not to an extent significant enough to warrant delaying surgery. Withholding clopidogrel is associated with an increase in the risk of cardiovascular complications such as MI or stroke. If the patient is high risk of bleeding then delaying surgery 24 hours from last dose allows time for clearance of residual clopidogrel (half life 6 hours), which allows transfusion of platelets if excessive bleeding occurs.
Dual Antiplatelet Therapy with Aspirin and Clopidogrel
- Stop clopidogrel on admission, continue aspirin. Plan surgery 24 hours from last dose of clopidogrel.
- Assume the patient to be at high risk of bleeding.
- These patients are likely to be at high risk of complications, both because bleeding risk is likely to be high and platelet and blood transfusions may be required, and additionally patients taking dual antiplatelets are usually at high risk of thrombosis. Continue aspirin and withhold clopidogrel. Delay surgery 24 hours from last dose of clopidogrel to allow clearance of residual drug, and this will allow transfusion of platelets if bleeding occurs. Delaying longer than 24 hours is likely to worsen outcome without significantly reducing bleeding risk. The risk of vertebral canal haematoma in patients taking dual antiplatelet agents is likely to outweigh any benefit from neuraxial anaesthesia in most patients.
Dual Antiplatelet Therapy with Aspirin and Other Antiplatelet Agent, e.g. ticagrelor, dipyridamole, prasugrel
- No guidance is available regarding bleeding risk for these drugs. Discuss with local haematologist or anaesthetist in the first instance.
High Risk Groups
Trauma Patient on Warfarin: Sample Action Plan
Content of this page adapted from the Anticoagulant consensus statement v1.0, 2018
Jonathan Antrobus, Consultant Anaesthetist, Borders General Hospital
Henry Watson, Consultant Haematologist, Aberdeen Royal Infirmary
Incorporating feedback from regional hip fracture governance teams, NHS Scotland. Consultation period June-Aug 2018